





Marc Darrow, MD.,JD.
If you’re dealing with a deep, persistent pain in your shoulder, you might have heard the term “SLAP tear.” It sounds a bit dramatic, but it’s a specific and common injury, especially for active people. A SLAP tear is an injury to the labrum, which is a ring of firm, flexible cartilage that lines your shoulder socket. Think of it as a rubber gasket that helps keep the head of your upper arm bone snug within the socket. This stability is crucial for the shoulder’s incredible range of motion. The term SLAP is an acronym for Superior Labrum Anterior and Posterior, which simply means the tear is located at the top part of the labrum, extending from the front to the back. This area is particularly important because it’s also where your biceps tendon attaches to the labrum. Recent, high-quality research has shown that for many patients, slap tear shoulder surgery- sometimes simply referred to as slap tear surgery- is no more effective than a placebo procedure. Before you commit to a long and difficult recovery process, it’s crucial to understand the full story. We’ll examine the data, discuss why these procedures have such mixed results, and explore non-surgical options that treat the entire shoulder to promote true healing.
Many emails that come in from this website, come from people asking about SLAP tear surgery. Some people want to know if they can avoid surgery. Some people are looking for options because they cannot get a SLAP tear surgery. Why can’t they get the surgery? Because their doctor/surgeon does not hold out good hope that surgery will be effective for them. Who are these people? From the emails we get, they are usually people with multi-directional shoulder instability, or, people who already had the surgery and despite it being a successful surgery, the person still had pain and range of motion issues. Before we get into the research, here is my story.
I have a labral tear in my right shoulder. I have a supraspinatus and subscapularis tear as well. I also have NO pain. How do I know I have the tears? Because I looked at my shoulder under ultrasound when I was having shoulder pain, one day especially, when I had a frozen shoulder from hitting too many golf balls. I am a very repetitive motion type athlete. I did have a shoulder surgery while I was in medical school. I had the orthopedic surgeon I was under perform it. The surgery was not successful. In fact, for me, it was terrible. The reason I got into this line of non-surgical medicine was because of the results I got in myself using regenerative medicine techniques. I have treated and healed my shoulder using Platelet Rich Plasma Therapy and Stem Cell Therapy. I’ve injected both my shoulders, both my knees, both my elbows, and wrist. This is not to say that this will work for everyone, but it worked for me.
“Neither labral repair nor biceps tenodesis had any significant clinical benefit over sham surgery for patients with SLAP II lesions in the population studied.”
In May 2017, A Norwegian research team lead by Dr Cecilie Piene Schrøder, an Orthopedic surgeon, examined the effectiveness of the routine surgical procedures they were performing for SLAP lesions or tears of the shoulder. Here is what the research team noted:(1)
- Labral repair and biceps tenodesis are routine operations for superior labrum anterior posterior (SLAP) lesion of the shoulder, but evidence of their effectiveness is lacking.
- We (the research team) evaluated the effect of labral repair surgery, biceps tenodesis surgery and sham (placebo) surgery on SLAP lesions.
So what Dr. Schrøder and his colleagues were looking for was to see if the surgeries they were performing actually worked by comparing them to a Sham or placebo surgery.
- They did a a double-blind, sham-controlled trial with 118 surgical candidates (average age 40 years), with patient history, clinical symptoms and MRI arthrography indicating an isolated type II SLAP lesion.
- Forty patients were randomly assigned to get a labral repair surgery.
- Thirty-nine patients received a biceps tenodesis surgery.
- Thirty-nine patients received a sham surgery.
- Results There were no significant between-group differences at any follow-up in any outcome.
- Conclusion Neither labral repair nor biceps tenodesis had any significant clinical benefit over sham surgery for patients with SLAP II lesions in the population studied.
In a 2025 paper (2) citing this research, doctors looked at the nocebo effect, “a phenomenon wherein negative expectations can worsen symptoms.” What the researchers found was a negative aspect was taken by patients who felt they were given diagnostic labels, had diagnostic imaging and special tests, and simply the actual occurrence of overtreatment or the perception that they were getting too much medicine.
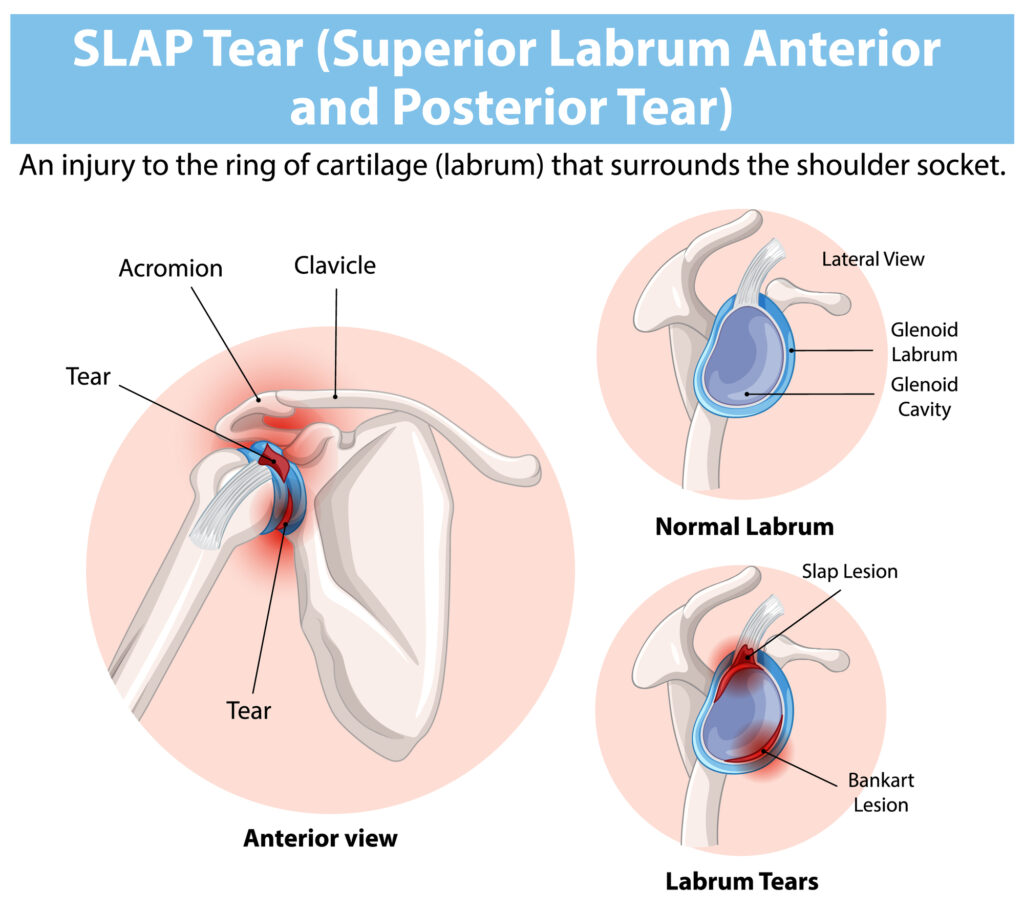
Understanding SLAP Tears: Anatomy, Causes, and Symptoms
To really get what a SLAP tear is, let’s picture your shoulder joint. It’s a ball-and-socket joint, with the “ball” being the top of your arm bone (the humerus) and the “socket” being a shallow dish on your shoulder blade (the glenoid). The labrum deepens this socket, acting like a bumper to keep the ball centered and secure. It also serves as an anchor point for several ligaments and, most notably for SLAP tears, the long head of the biceps tendon. When the top part of this labral ring tears, it can disrupt the stability of the joint and affect the biceps tendon, leading to the pain and dysfunction that many people experience.
What Causes a SLAP Tear?
So, how does this important piece of cartilage get torn? The causes of a SLAP tear generally fall into two buckets: a single, sudden injury or gradual wear and tear over time. A traumatic event can easily cause a tear, but so can the slow, repetitive stress from certain activities. Understanding the cause can sometimes help in determining the best path forward for treatment. For many, the injury isn’t from one memorable moment but rather the result of years of use, which can make pinpointing the exact origin a bit tricky. It’s a common issue for both athletes and non-athletes alike.
Acute Injuries vs. Repetitive Motion

Acute injuries that can cause a SLAP tear often involve a direct force to the shoulder. This could be from a fall onto an outstretched arm, a sudden pull when trying to lift a heavy object, or a direct impact like you’d get in a car accident or a contact sport. On the other hand, repetitive motion is a more common culprit, especially for overhead athletes like baseball pitchers, tennis players, and swimmers. The repeated overhead motion can gradually fray and weaken the labrum until it eventually tears. This type of wear-and-tear injury is also common in middle-aged individuals simply from years of daily activities.
Common Symptoms of a SLAP Tear
The signs of a SLAP tear can be a bit vague and often overlap with other shoulder problems, but there are a few classic symptoms to watch for. Many people report a feeling of locking, popping, catching, or grinding in the shoulder during movement. You might also feel a deep, aching pain inside the joint, which can be difficult to pinpoint. This pain often worsens when you lift objects, especially overhead, or when you hold your shoulder in specific positions. A decreased range of motion and a feeling of instability, as if your shoulder might pop out, are also common complaints. You may also notice a loss of strength in your shoulder.
How SLAP Tears Are Diagnosed and Conventionally Treated
Your journey to a diagnosis will almost always start with a conversation with your doctor about your symptoms and how the injury may have occurred. They’ll want to know what kind of pain you’re feeling, what movements make it worse, and if you’ve experienced any popping or catching sensations. This history can provide crucial clues. From there, your doctor will perform a physical exam to assess your shoulder’s strength, stability, and range of motion. This hands-on evaluation helps narrow down the potential sources of your pain and is a critical step before ordering any expensive tests.
Physical Exam and Imaging Tests
During the physical exam, your doctor may move your arm into various positions to see what causes pain or instability. They might perform specific maneuvers designed to stress the labrum and biceps tendon to see if they can reproduce your symptoms. If a SLAP tear is suspected based on the exam, the next step is often an imaging test. While an X-ray can rule out bone-related issues, an MRI may be recommended. MRIs readings are sometimes inaccurate in determining the degree of tear or sometimes they show a false positive. This is discussed in the ink below.
Common Nonsurgical Treatments
If you’re diagnosed with a SLAP tear, don’t assume surgery is your only option. In fact, most doctors will recommend trying nonsurgical treatments first, especially if the tear is minor or related to overuse. The primary goals of this approach are to manage your pain and inflammation while restoring strength and mobility to the shoulder. For many people, a dedicated course of conservative care is enough to get them back to their daily activities with significantly less pain. These methods focus on supporting the joint and allowing the inflammation to subside, which can make a huge difference in your symptoms.
Physical Therapy, Rest, and Anti-Inflammatories
The cornerstone of nonsurgical treatment is often a combination of rest, anti-inflammatory medications, and physical therapy. Over-the-counter drugs like ibuprofen or naproxen can help reduce pain and swelling. However if these treatments fail, you may be recommend to a physical therapy. For many people, failure of physical therapy to improve their condition results in a surgical recommendation.
Corticosteroid Injections
If oral anti-inflammatories and physical therapy aren’t providing enough relief, your doctor might suggest a corticosteroid injection. A powerful anti-inflammatory medication is injected directly into the shoulder joint to calm down severe pain and swelling. While these injections can be very effective for short-term pain relief, it’s important to understand that they don’t heal the torn labrum. They simply treat the symptoms. Because of this, their effects can be temporary. While they can provide a window of relief to make physical therapy more tolerable, some patients seek out regenerative medicine treatments that aim to support the body’s own healing mechanisms for a more foundational approach.
An Overview of SLAP Repair Surgery
When nonsurgical treatments don’t provide lasting relief, or if the tear is particularly severe, your doctor may bring up the possibility of surgery. The most common procedure for a SLAP tear is an arthroscopic repair. This is a minimally invasive surgery where the surgeon works through small incisions using a tiny camera and specialized instruments. The goal is to either repair the torn labrum by reattaching it to the bone or, in some cases, to address the biceps tendon if it’s also involved. While surgery is often presented as a definitive fix, it’s a major undertaking with a significant recovery period and its own set of potential risks and outcomes that are important to consider.
How the Arthroscopic Procedure is Performed
During an arthroscopic SLAP repair, the surgeon makes a few small portals, or cuts, around your shoulder. A small camera called an arthroscope is inserted through one portal, allowing the surgeon to see the inside of your joint on a monitor. Tiny surgical tools are inserted through the other portals to perform the repair. The surgeon will first inspect the labrum to confirm the extent of the tear. If a repair is possible, they will debride, or clean up, the frayed edges of the tear. Then, they will use small anchors with sutures attached to stitch the torn labrum securely back to the rim of the shoulder socket.
The Recovery and Rehabilitation Process
The recovery from SLAP repair surgery is often a long and challenging process that requires a great deal of patience and dedication. It’s not a quick fix; rehabilitation is just as important as the surgery itself. Immediately after the procedure, your arm will be immobilized in a sling to protect the repair and allow the labrum to begin healing to the bone. You’ll be given instructions on how to manage pain and swelling. The full recovery process is a gradual one, with specific milestones you’ll need to hit before you can safely return to all your normal activities, especially sports.
Timeline for Returning to Activities
The timeline for recovery can vary, but you can generally expect to be in a sling for about four to six weeks. During this time, you’ll likely start passive range-of-motion exercises with a physical therapist to prevent your shoulder from getting too stiff. After the sling comes off, you’ll begin a more active physical therapy program for several months to rebuild your strength and restore your mobility. It can take anywhere from four to six months to get back to most activities and potentially up to a year before you can return to high-level, overhead sports. This lengthy timeline is a major factor to weigh when considering surgery.
Potential Risks & Slap Tear Surgery Success Rate
Like any surgical procedure, SLAP repair comes with potential risks. While arthroscopic surgery is less invasive than open surgery, complications can still occur. It’s also important to have realistic expectations about the outcome. Research has shown that the slap tear surgery success rate is around 70%, meaning that a significant number of patients may not experience the complete pain relief and functional improvement they were hoping for. This is why it’s so important to have a thorough discussion with your surgeon about the potential benefits and drawbacks before making a decision and to explore all your options.
General Surgical Risks and When to Call a Doctor
The general risks associated with SLAP repair surgery include infection, bleeding, blood clots, and potential damage to the surrounding nerves or blood vessels. Another common issue after shoulder surgery is stiffness, or a “frozen shoulder,” which can require extensive physical therapy to resolve. After your procedure, you should contact your doctor if you experience signs of infection like fever, chills, or increasing redness and drainage from your incisions. It’s also important to report any new numbness or tingling in your arm or hand, as this could indicate nerve issues. Being aware of these potential complications is a key part of the surgical process.
Why Most SLAP Lesions Don’t End in Surgery
In July 2018, Dr. Schrøder followed up his paper we spoke of above with a short piece published in the The open orthopaedics journal. Here he addressed criticism about his findings. When questioned on the usefulness of SLAP tear surgery, Dr. Schrøder responded: “Based on (our) results we have narrowed our indications for SLAP lesion surgery. We still treat some SLAP lesions surgically and individualize our treatment in each such cases. Most SLAP lesion patients, however, are ultimately treated non-operatively.”(3) Another 2018 study, this time from Department of Orthopaedic Surgery, Stanford University (4) found that “The management of Type-II superior labral tears (SLAP) of the shoulder remains a controversial topic. Treatment ranges from non-operative management to surgical management including SLAP repair, biceps tenotomy, and biceps tenodesis. An optimal treatment algorithm has yet to reach universal acceptance.” These researchers suggested: “Management of Type-II SLAP tears remains a diagnostic and therapeutic challenge, especially in the context of lack of consensus in the literature. Surgical management includes labral repair, biceps tenodesis, biceps tenotomy, or a combination. Clinical decision making should be based on patient age, desired activity levels, the degree of participation in overhead sports, and the presence or absence of other associated pathology. These variables should be considered carefully as the surgeon and patient develop the ideal surgical treatment plan after conservative measures have failed.”
SLAP Repair: Why Even Experts Report Mixed Results
A January 2018 study from the Hospital of Special Surgery and the Mayo Clinic discussed the diagnostic and treatment challenges presented by injuries to the biceps and superior labral complex. “Nonoperative management, even in overhead athletes, has demonstrated relatively good outcomes, while operative outcomes have yielded mixed results. The surgeon must take into account a number of variables when choosing the appropriate surgical procedure: labral repair versus biceps tenodesis. Rehabilitation, either as nonoperative management or as a postoperative protocol, should focus on restoring glenohumeral and scapulothoracic strength, endurance, and full, pain-free range of motion, while correcting any deficiencies in balance or rhythm throughout the overhead motion.”(5) A bicep tenodesis is a surgery to repair a damaged bicep tendon. A biceps tenodesis may be performed as an isolated procedure but more often is part of a larger shoulder surgery, including rotator cuff repair. A recent study from Rush University Medical Center warns of including this procedure during the bigger shoulder surgery: “High-demand patients with biceps tendonitis in the setting of a SLAP lesion with labral instability who undergo combined tenodesis and SLAP repair have significantly worse outcomes than patients who undergo either isolated labral repair for type II SLAP tears or isolated biceps tenodesis for a SLAP tear and biceps tendonitis.”(6)
Does More Shoulder Surgery Lead to Worse Outcomes?
The surgical treatment of SLAP tears continues to be challenging for both the physician and the patient. Of course it becomes much more challenging to the patient if the surgery does not work to the patient’s expectations. Here is a recent paper discussing these problems from doctors at the University of Minnesota and Saarland University in Germany.
- Tears of the superior labrum involving the biceps anchor are a common entity, especially in athletes, and may highly impair shoulder function. If conservative treatment fails, successful arthroscopic repair of symptomatic SLAP lesions has been described in the literature particularly for young athletes.
- However, the results in throwing athletes are less successful with a significant amount of patients who will not regain their pre-injury level of performance (see below for further documentation).
- The clinical results of SLAP repairs in middle-aged and older patients are mixed, with worse results and higher revision rates as compared to younger patients. In this population, tenotomy or tenodesis of the biceps tendon (doctors will move the bicep tendon attachment to a different place on the bone – usually part of a more major surgery) is a viable alternative to SLAP repairs in order to improve clinical outcomes. (7)
What Happens When SLAP Tear Surgery Fails?
A study from July 2018 in the The open orthopaedics journal (8) throws a lot of questions at the effectiveness of SLAP tear surgery.
- “Optimal treatment of type II superior labrum anterior and posterior (SLAP) tears is controversial. There has been a recent trend towards biceps tenodesis over SLAP repair in older patients. Few surgeons have performed combined biceps tenodesis and SLAP repair with inferior results.”
- “Failed SLAP repair is often multifactorial and a thorough workup is needed. Combined biceps tenodesis and SLAP repair can cause pain, stiffness, and dysfunction which can be successfully treated with arthroscopic superior capsular release.”
Why Revision Surgery Often Fails After a SLAP Repair
Similar findings were observed by surgeons at New York University Hospital for Joint Diseases. They found that on average 10% of patients would need a second shoulder surgery at average two years after the initial SLAP lesion procedure and those procedures were expanded to include subacromial decompression (35%), debridement (26.7%). repeat SLAP repair (19.7%), and biceps tenodesis or tenotomy (13.0%). After isolated SLAP repair, patients aged 30 Years or younger were more likely to undergo arthroscopic Bankart repair. The doctors concluded: “We identified a 10.1% incidence of subsequent surgery after isolated SLAP repair, often related to an additional diagnosis, suggesting that clinicians should consider other potential causes of shoulder pain when considering surgery for patients with SLAP lesions. In addition, the number of isolated SLAP repairs performed has decreased over time, and management of failed SLAP repair has shifted toward biceps tenodesis or tenotomy over revision SLAP repair in more recent years.(9) Also in the July 2018 edition of The open orthopaedics journal, (10) is another study that suggests that for many patients, SLAP tear surgery is not ideal. Risk factors for failure of SLAP repair include age, smoking, obesity, being female and concomitant bicep pathology(weakened, injured biceps). The researchers of this study cited a previous study that found that once a patient has failed first time repair, 71% will fail conservative therapy and 32% will continue to have suboptimal outcomes after a second surgical intervention.
Why Doctors Advise Athletes Against SLAP Surgery
Is shoulder surgery the only answer for the athlete who wants a quick return to their sport? To many athletes the answer is yes because the alternative recommendations from their orthopedic specialist of ice, rest, physical therapy and wait six months is not the option they want. Doctors at Houston Methodist Hospital however made this recommendation in published research in the American Journal of Sports Medicine, “Nonsurgical treatment should be considered for professional baseball players with documented SLAP lesions, as it can lead to acceptable RTP (Return-to-play) and RPP (return to prior performance (before injury)) rates.”(11) For many, many years before these studies, patients came into the office and would tell us about their shoulder labrum tear and the surgery they had, and the pain they still suffer from, and their desperation not to have another surgery. After talking with the patient we discover that a torn labrum showed up on an MRI, the surgery was performed, but, the pain never went away. Something else was causing the pain. As suggested above in why the surgery fails at higher rate and secondary revision is equally prone to failure is that patient may not even have a Slap tear.
Are SLAP Lesions Being Overdiagnosed?
Recently when Stephen C. Weber, MD presented the findings of his study that American Board of Orthopaedic Surgery (ABOS) Part II candidates (young surgeons) may be performing superior labral tear anterior to posterior (SLAP) repairs at greater rates than they should, he noted that the increase in surgeries were leading to poor outcomes and increased complication rates. One of the reasons too many surgeries were being performed was because MRI suggested a SLAP tear when Slap tears were not there. Dr. Weber noted that magnetic resonance imaging (MRI) scans often produce false positives and that SLAP lesions are difficult to diagnose clinically. Numerous studies suggest that even experts disagree on how to define a type II SLAP tear. “Furthermore, repairing SLAPs is not a benign process, and caring for failed SLAPs can be very difficult,” said Dr. Weber. “Complications include stiffness, persistent rotator cuff tears next to the portals, and damage to the articular cartilage.”
To Treat a SLAP Tear, You Must Treat the Whole Shoulder
SLAP lesions do not happen overnight unless you take a fall with your arm extended. Then you can have an acute tear. More typically SLAP lesions occur as the result of repetitive motion or wear and tear injury. SLAP lesions, therefore, do not happen in isolation, they happen as part of a degenerative shoulder disease problem. People who email me typically describe that they have a SLAP tear as well as a torn tendon, torn rotator cuff muscles, and chronic shoulder instability, sometimes with dislocation.The have all the symptoms of a shoulder that is in a downward spiral: Pain and a lot of noise, clicking, grinding, and popping. They have limited range of motion and a significant decrease in strength. It is for these reasons that shoulder surgery for SLAP tears and lesions is not effective. The surgery does not address the whole shoulder problem. Stem cells and Platelet Rich Plasma Therapy are injection techniques that can accelerate the body’s own inflammatory response to repair the labral damage. But treating the whole shoulder capsule, we can not only repair the labrum, but we can also protect it from damage and shoulder instability caused by compromised shoulder structures, such as ligaments and tendons. By treating the whole shoulder, we can strengthen these weakened elements and stabilize the entire joint.
References
1 Schrøder CP, Skare Ø, Reikerås O, Mowinckel P, Brox JI. Sham surgery versus labral repair or biceps tenodesis for type II SLAP lesions of the shoulder: a three-armed randomised clinical trial. British Journal of Sports Medicine. 2017;51(24):1759-1766. doi:10.1136/bjsports-2016-097098.
2 Lluch-Girbés E, Dueñas L, Struyf F, Camerone EM, Rossettini G. Negative expectations and related nocebo effects in shoulder pain: a perspective for clinicians and researchers. Pain management. 2025 Feb 1;15(2):93-104.
3 Schrøder CP. SLAP lesions, An Opinion Piece. The Open Orthopaedics Journal. 2018;12:342-345. doi:10.2174/1874325001812010342.
4 Johannsen AM, Costouros JG. A Treatment-Based Algorithm for the Management of Type-II SLAP Tears. Open Orthop J. 2018 Jul 31;12:282-287. doi: 10.2174/1874325001812010282. PMID: 30197709; PMCID: PMC6110057.
5 Calcei JG, Boddapati V, Altchek DW, Camp CL, Dines JS. Diagnosis and Treatment of Injuries to the Biceps and Superior Labral Complex in Overhead Athletes. Current Reviews in Musculoskeletal Medicine. 2018:1-9.
6 Chalmers PN, Monson B, Frank RM, Mascarenhas R, Nicholson GP, Bach BR, Verma NN, Cole BJ, Romeo AA. Combined SLAP repair and biceps tenodesis for superior labral anterior–posterior tears. Knee Surgery, Sports Traumatology, Arthroscopy. 2016 Dec 1;24(12):3870-6.
7 Brockmeyer M, Tompkins M, Kohn DM, Lorbach O. SLAP lesions: a treatment algorithm. Knee Surg Sports Traumatol Arthrosc. 2016 Feb;24(2):447-55. doi: 10.1007/s00167-015-3966-0. Epub 2016 Jan 27.
8 Han Y, Lee J, Park S, Suh E. Suppl-1, M5: Superior Capsular Release After Failed Combined Superior Labral Repair And Biceps Tenodesis For Slap Tear. The open orthopaedics journal. 2018;12:295.
9 Mollon B, Mahure SA, Ensor KL, Zuckerman JD, Kwon YW, Rokito AS. Subsequent shoulder surgery after isolated arthroscopic SLAP repair. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2016 Oct 31;32(10):1954-62.
10 Charles MD, Christian DR, Cole BJ. Suppl-1, M2: An Age and Activity Algorithm for Treatment of Type II SLAP Tears. The open orthopaedics journal. 2018;12:271.
11 Fedoriw WW, Ramkumar P, McCulloch PC, Lintner DM. Return to play after treatment of superior labral tears in professional baseball players. Am J Sports Med. 2014 May;42(5):1155-60. doi: 10.1177/0363546514528096. Epub 2014 Mar 27.
Marc Darrow, M.D., J.D., is one of the world’s most experienced Regenerative Medicine doctors. He has more than 30 Years of expertise in regenerative medicine techniques and has treated thousands of patients. He uses non-surgical therapy to reduce pain in joints, tendons, ligaments, and a variety of other ailments and disorders throughout the body, including back and neck discomfort. He taught at UCLA and received Board Certification in Physical Medicine and Rehabilitation.